This case study highlights a Northern California based healthcare system, which includes more than 24 acute care hospitals and 200 clinics. Like many systems, optimal patient care is a priority; however, their approach is unique in its focus on an integrated, team-based approach bolstered by the adoption of innovative technologies.
There’s no better benefit than being right.”
– Brad Angeja, MD, Cardiologist
Featured Videos
Cardiologist & Radiologist Perspectives
Case Reviews with Dr. Brad Angeja
The Mainstream Approach
The traditional approach guiding coronary artery disease (CAD) diagnosis and management relies primarily on stress testing—despite widely recognized shortcomings—costing billions of dollars globally every year due to missed diagnoses and unnecessary diagnostic testing. Diagnosing CAD is often subject to interpretation, highly variable, and particularly vulnerable to snap judgement decisions when made during an invasive procedure.
20% to 30% false negatives from stress tests1
55% false positives from CT tests, often resulting in unnecessary diagnostic angiograms2
Incomplete information results in layered testing, repeat patient visits and overuse of resources
We joke that nuclear medicine is unclear medicine, because the images are blurry. CT with the HeartFlow Analysis brings the diagnosis into focus. I feel like I’m putting on glasses and seeing better, and it’s a great feeling.”
– Brad Angeja, MD, Cardiologist
A Clearer Path - CTA + HeartFlow
Realization of a successful CTA + HeartFlow program impacts not only patient outcomes, but also operational efficiency and program success. Patients and staff benefit from a “one stop, closed loop test” that encourages dialogue between specialties, improves overall CT quality and interpretation, and beyond making a more accurate diagnosis, provides powerful risk stratification and prognostic information that helps guide medical therapy strategies.
Higher diagnostic accuracy using a CTA + HeartFlow pathway3
98% negative predictive value from CTA4
Physiology information that improves anatomic data accuracy
Impact of blockages on blood flow
Less time, risk, radiation/COVID-19 exposure for patients/staff
We’ve seen literally hundreds of studies that prove that coronary CT is not just a problem solving tool but really is the most powerful firstline diagnostic test for the workup of coronary artery disease. What the HeartFlow Analysis brings to coronary CT is the ability to understand what a blockage means.”
– Eric Flagg, MD, Radiologist
Availability of the HeartFlow Analysis
One of the striking differences between the HeartFlow Analysis compared to other tests is the quality and clarity of data provided in a simple-to-read, interactive 3D model of a patient’s coronary arteries. Interpretation is simplified and impact to patient education is transformed.
Keys to Success
Leading with a focus on “what’s right for the patient” sets an important standard. With this goal in mind, identifying and trusting in a new, yet proven pathway is essential, as well as taking a multi-disciplinary, collaborative approach to adoption.
Establish a quality CTA program, in partnership with HeartFlow
Engage the entire clinical team to prioritize high quality CTA scans for the betterment of patient care
Prioritize sending CTA scans with a stenosis of 30-90%
Leverage the HeartFlow mobile app to see results right away while on the go
The key point where HeartFlow comes in is that it enhances the dialogue after the scan. The more robust the communication between specialties taking care of patients, the better the patient care that’ll be achieved.”
– Eric Flagg, MD, Radiologist
A Focus on Patient Care
With competing tests to choose from, deciding which one to use has historically been confusing. Shifting to a CTA + HeartFlow frontline strategy for patients presenting with symptoms of coronary artery disease, streamlines diagnosis, provides clarity and gives confidence to physicians and patients of the final treatment plan.
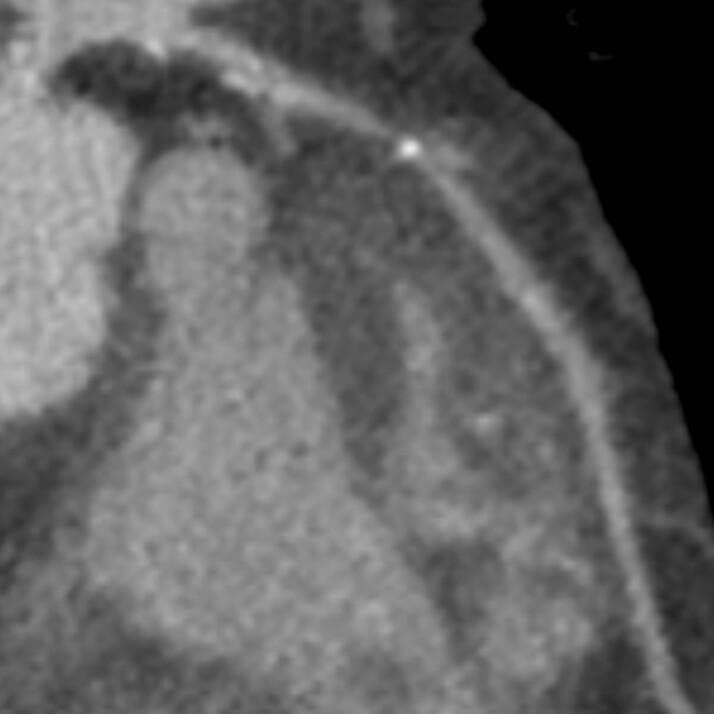
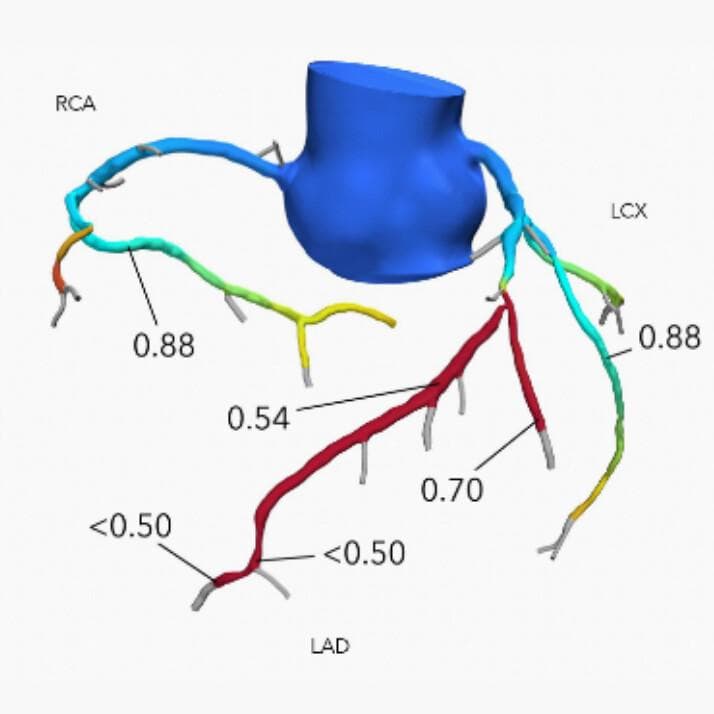
This is a common case in which an abnormal stress test would have resulted in a diagnostic angiogram to view the coronary arteries for the first time during the procedure. In contrast, CTA and HeartFlow provide precise anatomic and physiologic information indicating the impact blockages have on blood flow, which allows the interventionalist to pinpoint problem areas and plan a procedure in advance of the cath lab.
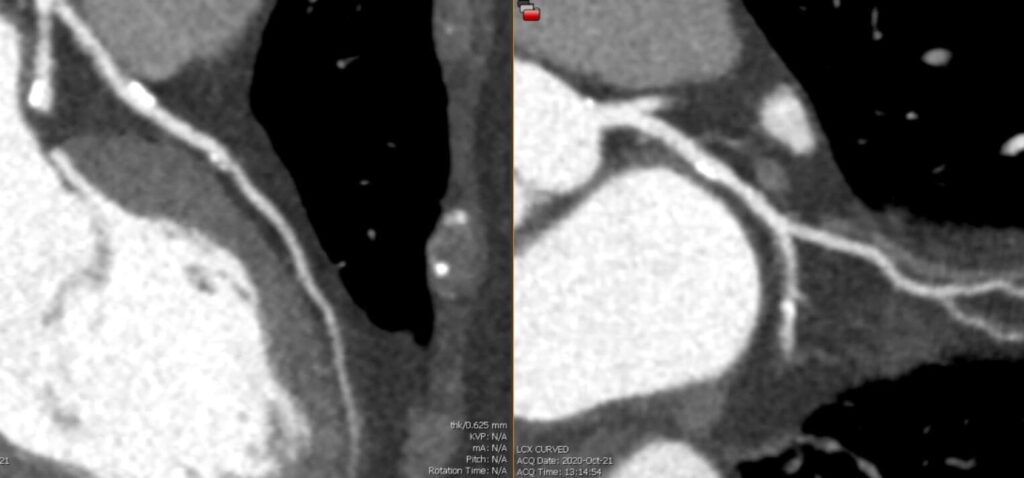
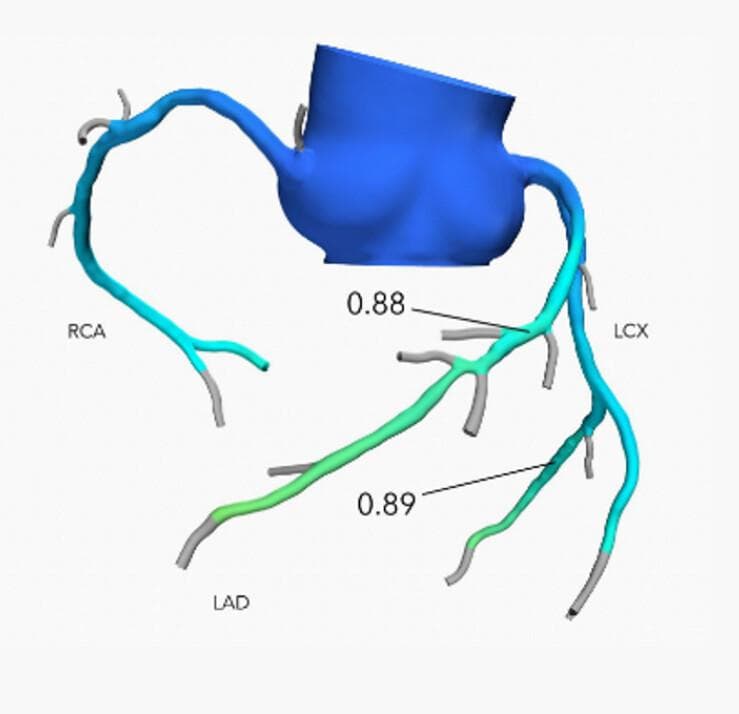
This is another common case, in which plaque seen on CTA would have led to an invasive diagnostic angiogram. Pairing CTA with the HeartFlow Analysis instead provides confidence that if the blockages are not flow limiting, as in this case, a patient can be safely treated medically, avoiding the resources and risks associated with invasive tests.
Patient History
68-year-old-man with high blood pressure, high cholesterol, and squeezing chest tightness while walking, starting 2 months prior.
The Results
LAD blockage confirmed
1 stent placed
Angina resolved
CTA
HeartFlow Analysis
Angiogram
Patient History
68-year-old-woman with positional chest pain and prior equivocal stress echo, then a normal nuclear scan.
Risk factors
Strong family history, former smoker, twin brother had a heart attack at age 53
High cholesterol; Not on statin
The Results
Ca score 500
Statin now prescribed
Mild-moderate LAD lesion
Confidence that revascularization is not needed
CTA
HeartFlow Analysis
I’ve had people come to me, excited about hearing that they can get a heart scan and have the ability to see their arteries and see the colors of the HeartFlow Analysis. From the standpoint of patient understanding, education, consent, adherence to therapy, I think they are much more engaged. It’s more clear for the patient, and we can achieve that without a half a day in the office or overnight stay, which provides a much better patient experience.”
– Brad Angeja, MD, Cardiologist
Doctors Angeja and Flagg are co-leads of the CT + HeartFlow program and are responsible for the expansion of the CTA program across numerous sites throughout their system.
Arbab-Zadeh, Heart Int 2012. Yokota, et al. Neth Heart J 2018. Nakanishi, et al. J Nucl Cardiol 2016.
Patel, et al. N Engl J Med 2010. Patel, et al. AHJ 2014. Danad, et al. JAMA Cardiology 2017.
Driessen, et al. J Am Coll Cardiol 2019.
Hoffmann, et al. J Am Coll Cardiol. 2009.
Contact Us
*Required fields
Request the HeartFlow Analysis Near You
If you would like to request to have the HeartFlow Analysis available at a location near you, please submit your information below with details of the institution. We will share this information with the institution, but it will not guarantee HeartFlow will become available.
*Required fields
残念ながら、GDPR 規制により、この Web フォームを通じて求人への応募やキャリアに関する問い合わせを受け付けることはできません。弊社を通じてお申込みください 採用ページ. ご関心をお寄せいただきありがとうございます!
The HeartFlow FFRCT Analysis is a personalized cardiac test indicated for use in clinically stable symptomatic patients with coronary artery disease by qualified clinicians. The information provided by the HeartFlow Analysis is intended to be used by qualified clinicians in conjunction with the patient’s history, symptoms, and other diagnostic tests, as well as the clinician’s professional judgement.
If you have additional questions, close out of this message to complete our form or call our support team: 877.478.3569.
Please use our online submission form on the Clinical Research Page to apply for research grants.
Thank you for your interest!
Unfortunately, we cannot take job applications or career inquiries through this web form due to GDPR regulations. Please apply through our Careers Page. Thank you for your interest!
Campbell Rogers, M.D., F.A.C.C.
Executive Vice President and Chief Medical Officer
Campbell brings a wealth of experience to HeartFlow, where he serves as the Chief Medical Officer. Prior to joining HeartFlow, he was the Chief Scientific Officer and Global Head of Research and Development at Cordis Corporation, Johnson & Johnson, where he was responsible for leading investments and research in cardiovascular devices. Prior to Cordis, he was Associate Professor of Medicine at Harvard Medical School and the Harvard-M.I.T. Division of Health Sciences and Technology, and Director of the Cardiac Catheterization and Experimental Cardiovascular Interventional Laboratories at Brigham and Women’s Hospital. He served as Principal Investigator for numerous interventional cardiology device, diagnostic, and pharmacology trials, is the author of numerous journal articles, chapters, and books in the area of coronary artery and other cardiovascular diseases, and was the recipient of research grant awards from the NIH and AHA.
He received his A.B. from Harvard College and his M.D. from Harvard Medical School.