
Why Coronary Anatomy & Physiology Are Not the Same
First and foremost, I hope this note finds you and your families safe and healthy.
During this time, all of us have been involved in significant learning and reeducation efforts. This may mean cross-training in the ED or ICU, refocusing on system-wide planning, or simply adopting new ways to communicate with patients.
Like many of you, I have been using this time to participate and learn from online webinars. Professor Nick Curzen, chair of interventional cardiology at the University of Southampton and president of the British Cardiovascular Intervention Society, and Dr. Jonathon Leipsic1, a cardiac-focused radiologist in Vancouver, BC and past president of the Society of Cardiovascular CT, led a very informative session discussing the data and clinical experience which demonstrate the need for cardiologists to appreciate the differences between coronary anatomy and physiology and to understand the need to incorporate both elements in decision-making.
Several points stood out to me as Prof. Curzen and Dr. Leipsic comprehensively reviewed the vast clinical literature on this topic including study data on thousands of patients:
- Anatomical discordance is pervasive. Pooling over 6,600 invasive FFR measurements from FAME and other major studies shows that in at least 30% of coronary lesions, anatomic severity does not predict physiology.2 While this is widely reported in anatomically intermediate (50-70%) lesions, it is clear that physiologic discordance commonly occurs across a far wider range of anatomical lesions (30-90%).“It’s good to know the anatomy because then you know that they will benefit prognostically from disease modifying therapy. But if you’re looking to decide which patient and which artery and which lesion needs revascularization, then you need to know the physiology.” – N. Curzen
- Physiology informs clinical decisions. In multiple studies where clinicians reported treatment plans (1) after observing anatomy via angiography or coronary CTA and (2) again when lesion-specific physiologic information became available, it was shown that knowing the physiology (invasive or non-invasive) caused clinicians to alter treatment plans in 30-50% of cases.3“[With physiologic information], the treatment was changed and it was changed in all different directions. So some medical patients then needed revasc, some people who needed PCI were changed to medical, some people who needed bypass surgery based on the angiogram needed medical, et cetera, et cetera.” – N. Curzen
- Using both improves outcomes. A recent registry with nearly 18,000 patients from the US Veterans Affairs (VA) Health System found that FFR-guided revascularization was associated with a 43% reduction in all-cause mortality within a year relative to angiographic-only guided revascularization. Use of FFR for lesions of intermediate severity was shown to have nearly doubled from 44% (2010) to 75% (2017).4“Guiding revascularization, not on the basis of the severity of the stress test abnormality, as we saw in the ISCHEMIA trial, and not based on anatomy from CT or invasive angiography, but rather with invasive physiology or a measure of physiology is what’s really needed.” – J. Leipsic
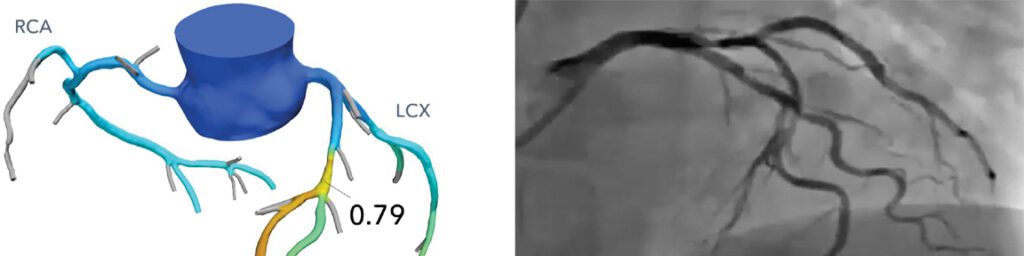
These clear improvements in clinical outcomes that result from applying physiology to clinical decision making is at the heart of why physicians have chosen the HeartFlow FFRct Analysis for over 50,000 patients.
If you would like to review some of the highlights of this session, or the session in its entirety, you can find the link here. I am confident you will find insights that will impact your daily clinical work.
— A perspective from HeartFlow Chief Medical Officer, Campbell Rogers, MD
Bio | LinkedIn
1. Dr. Leipsic also serves as a paid consultant to HeartFlow providing guidance on medical education and science.
2. Curzen, et al. Circ Interven 2014. Tonino, et al. J Am Coll Cardiol 2010. Berry, et al. Euro Heart J 2014. Toth, et al. Euro Heart J 2014.
3. Curzen, et al. Circ Interven 2014. Curzen, et al. J Am Coll Cardiol Img 2016. Patel, et al. J Am Coll Cardiol Img 2019.
4. Parikh, et al. J Am Coll Cardiol 2020.

