Cone Health is one of the nation’s premier heart and vascular care centers due in part to its commitment to continuous improvement and investment in innovative technologies that improve patient care. The Cone Health team identified opportunities to streamline testing, achieve efficiencies in cath lab processes and improve the patient journey by reducing its reliance on stress testing for diagnosis of coronary artery disease. In seeking the most advanced solutions, the Cone Health team found HeartFlow in 2017.
As an early adopter of the CCTA-first pathway coupled with the HeartFlow Analysis, their cardiovascular program continues to demonstrate leadership in advancing the quality of heart and vascular care for patients. Hear key members of the Cone Health team discuss why they adopted the HeartFlow Analysis, the impact it’s had on patient care and key components of the program’s success in our latest case study.
Sheryl Booth
Executive Director Heart & Vascular
Dr. Katarina Nelson
CT Program Lead, Imaging Cardiologist
Dr. Henry Smith
Interventional Cardiologist
Sara Wallace
Nurse Navigator
“Looking at it from the broad overview that I have, we have a huge list of benefits that go along with having this technology.”
“The HeartFlow Analysis complements our anatomical images from Coronary CT with functional information, and it also helps procedural planning for the interventional cardiologists.”
“I am impressed by the high sensitivity and specificity that the HeartFlow Analysis brings to the management of patients with coronary artery disease and stable chest pain.”
“It’s really amazed me how much I’ve learned in the last few months about this technology and how the HeartFlow Analysis combines anatomy and function.”
Sheryl Booth
Executive Director Heart & Vascular
“Looking at it from the broad overview that I have, we have a huge list of benefits that go along with having this technology.”
Dr. Katarina Nelson
CT Program Lead, Imaging Cardiologist
“The HeartFlow Analysis complements our anatomical images from Coronary CT with functional information, and it also helps procedural planning for the interventional cardiologists.”
Dr. Henry Smith
Interventional Cardiologist
“I am impressed by the high sensitivity and specificity that the HeartFlow Analysis brings to the management of patients with coronary artery disease and stable chest pain.”
Sara Wallace
Nurse Navigator
“It’s really amazed me how much I’ve learned in the last few months about this technology and how the HeartFlow Analysis combines anatomy and function.”
Limitations of the Traditional Care Pathway
Limitations of the Traditional Care Pathway
By initially relying on stress tests, such as SPECT and stress echo, with Coronary Computed Tomography Angiography (CCTA) alone used as backup, the Cone Health team experienced typical rates of false positives and false negatives. The team set three key improvement goals: reduce the number of tests required of patients, reduce diagnostic caths and identify patients at-risk of recurring chest pain earlier. By achieving these goals, Cone Health anticipated a reduction in radiation exposure for patients and care teams, improved cath lab efficiencies, better utilization of resources and a reduction in costs for both the health system and patients.
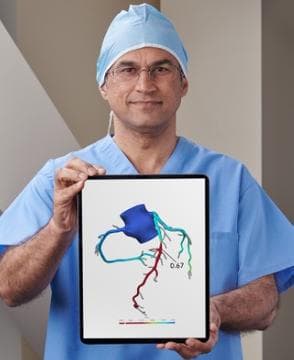
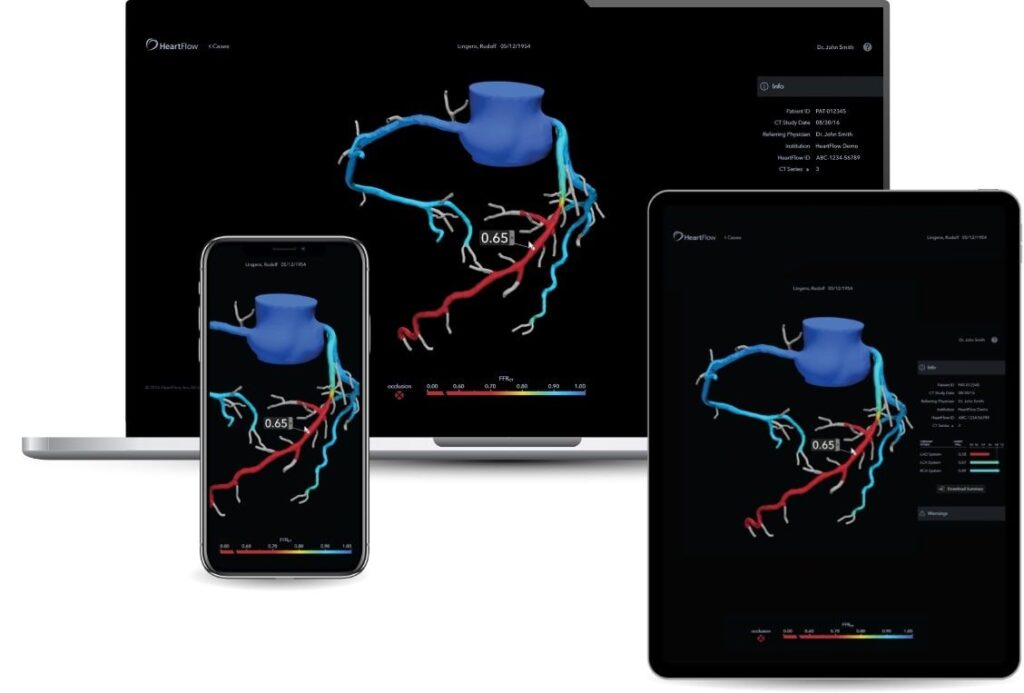
The HeartFlow Analysis is a non-invasive diagnostic test that helps physicians identify the impact that blockages have on blood flow to the heart. By leveraging a standard CT, the latest advancements in AI, cloud computing and computational physiology, physicians get both anatomic and physiologic information in one test. This powerful combination of information allows physicians to clearly identify problem areas before entering the cath lab. The results are presented as a color-coded 3D model of a patient’s arteries and are available as a web application via desktop or mobile. This technology enabled the Cone Health team to better triage patients without the capital expense or investment often required when adopting new technology.
“We were early adopters of technology that enables more comprehensive evaluation of coronary artery disease by providing both anatomical and functional information and improves patients’ outcomes.”
— Katarina Nelson, MD
CT Program Lead, Imaging Cardiologist
Accuracy
Traditional diagnostic tests result in 20-30% false-negative rates1 and 55% false positive rates2. In contrast, CT has a 98% negative predictive value3 allowing physicians to safely defer patients without disease, and when 30-90% disease is present and more information is needed, HeartFlow helps fill in the gaps by providing functional information. The HeartFlow Analysis is proven to have the highest diagnostic performance over other non-invasive tests with long-term outcomes out to five years. For the Cone Health team this translates to appropriate use of the cath lab for interventional procedures that are more predictable, well planned, coordinated and discussed with patients and the entire care team in advance of procedures.
“This gave me a tool that I felt was more trustworthy and helped to get away from the high false positives we were getting with SPECT.”
— Henry Smith, MD
Interventional Cardiologist
Patient Care
Patient satisfaction has become an integral component of a value-based healthcare system, and adoption of innovative technologies can help support meeting these goals. With the HeartFlow Analysis, patients avoid the amount of time, money and anxiety that would have resulted from using other tests and instead benefit from an accurate diagnosis and a clearer understanding of their heart health. The Cone Health team now has more engaged patient-provider conversations which helps put patients at the center of their care and build trust in the entire process.
“By having a structured program with a dedicated team, you can create a better workflow and patient experience.”
— Sheryl Booth, RT(R), MHA
Executive Director Heart & Vascular
HeartFlow Analysis Patient Case
Patient Summary
Age: 68 Sex: Male History: Hypertension, long standing tobacco use, obesity, squamous cell lung cancer and left upper lobe resection in 2014, and obstructive sleep apnea who was referred to cardiology for progressively worsening shortness of breath after coronary calcifications were noted on follow up surveillance chest CT.
Coronary CTA
Calcium score was 606 Agatson units that placed the patient in the 80th
percentile for age and gender suggesting high risk for future cardiac events.
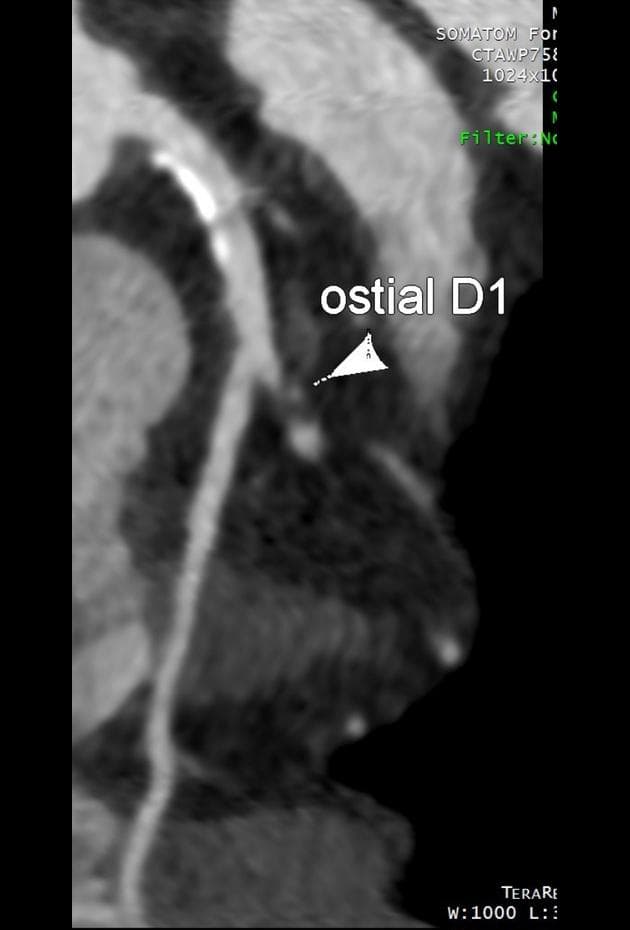
Calcifications were found diffusely in all three coronary arteries.
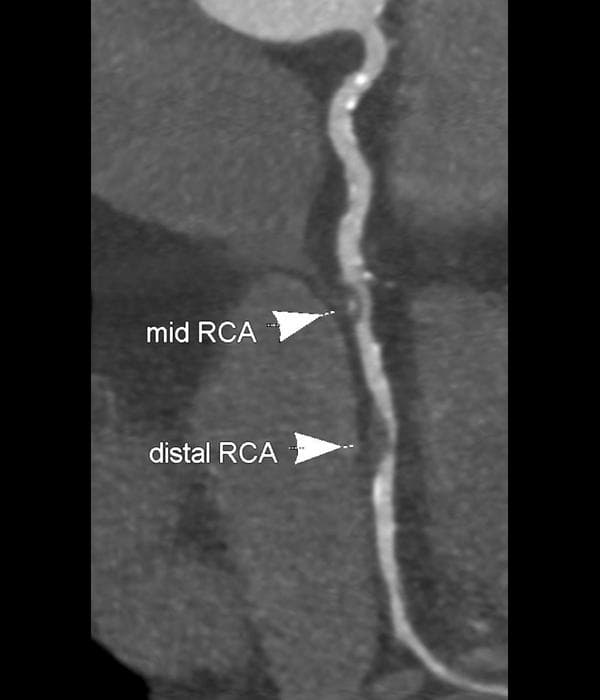
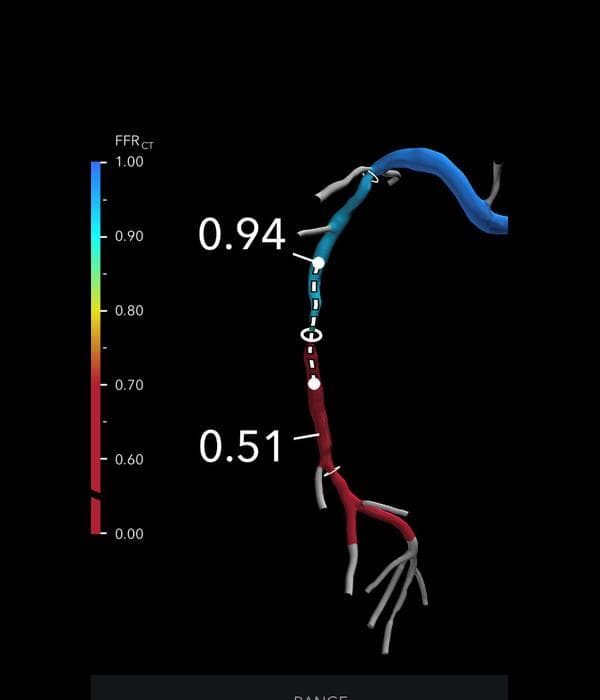
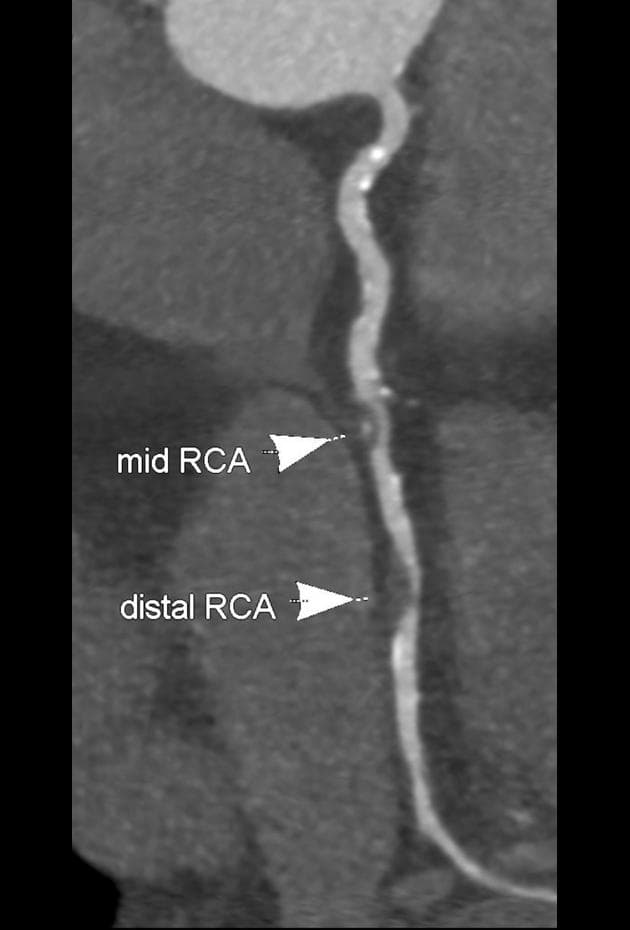
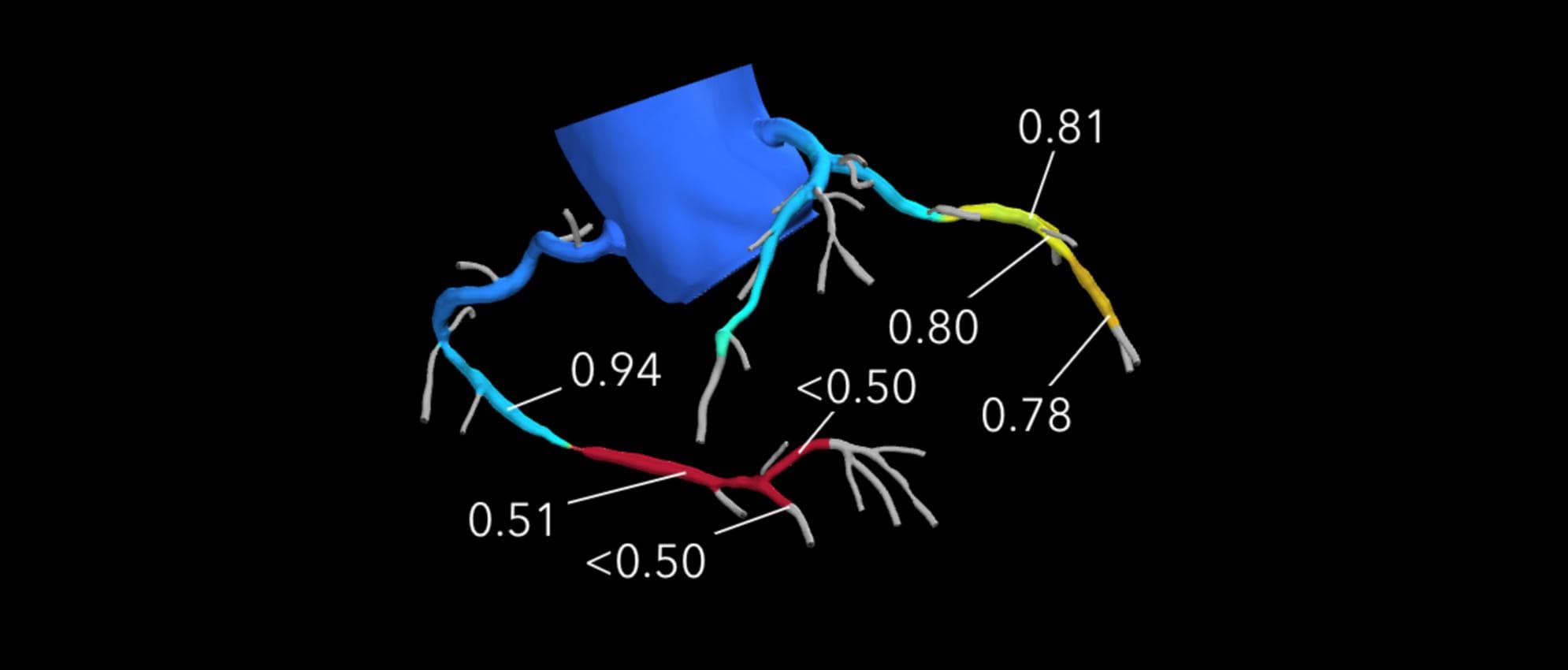
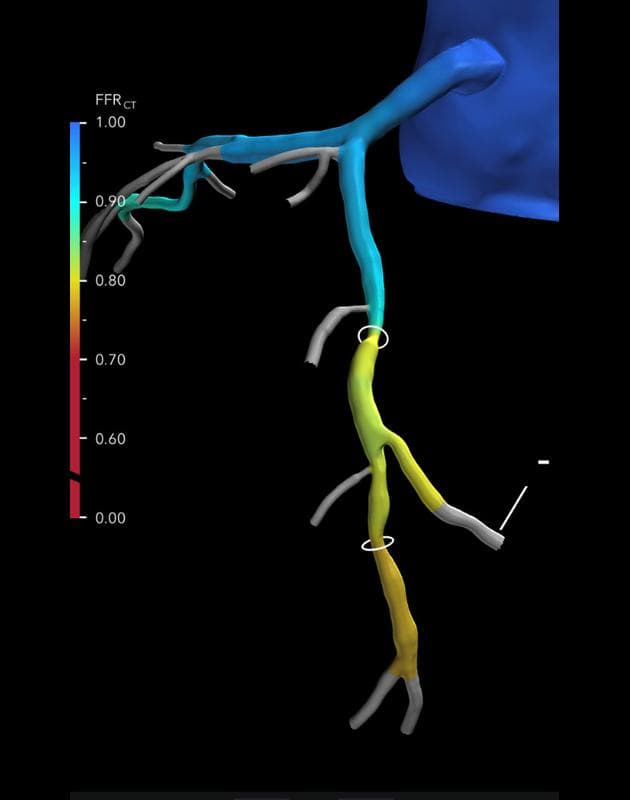
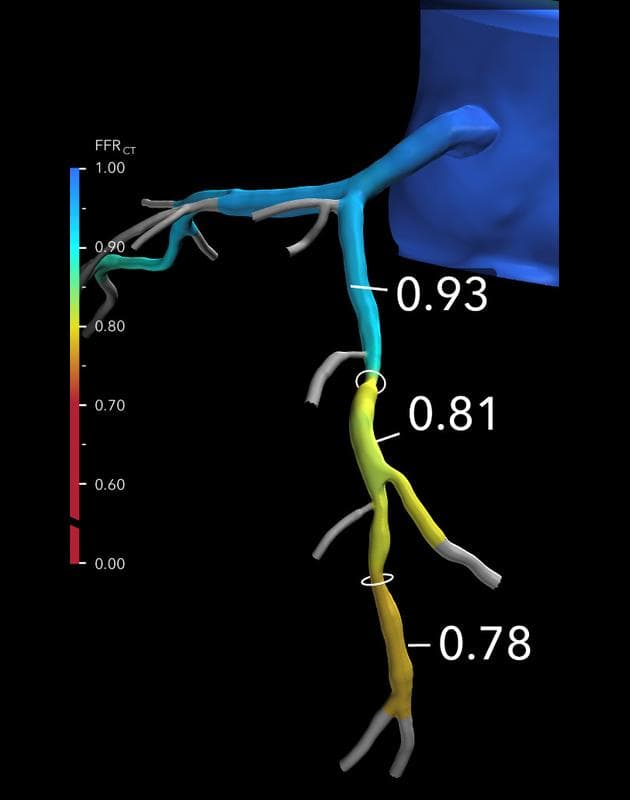
HeartFlow FFRCT Analysis
The HeartFlow Analysis allowed the physician to identify functionally significant disease in the mid and distal Right Coronary Artery (RCA) with a .51 FFRCT, in addition to diffuse, restricted blood flow in the Left
Circumflex Artery (LCX).
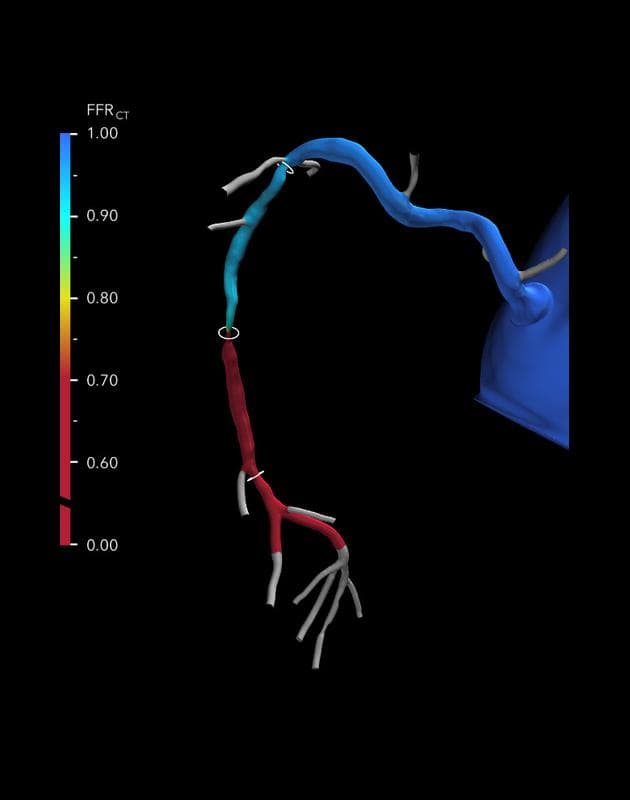
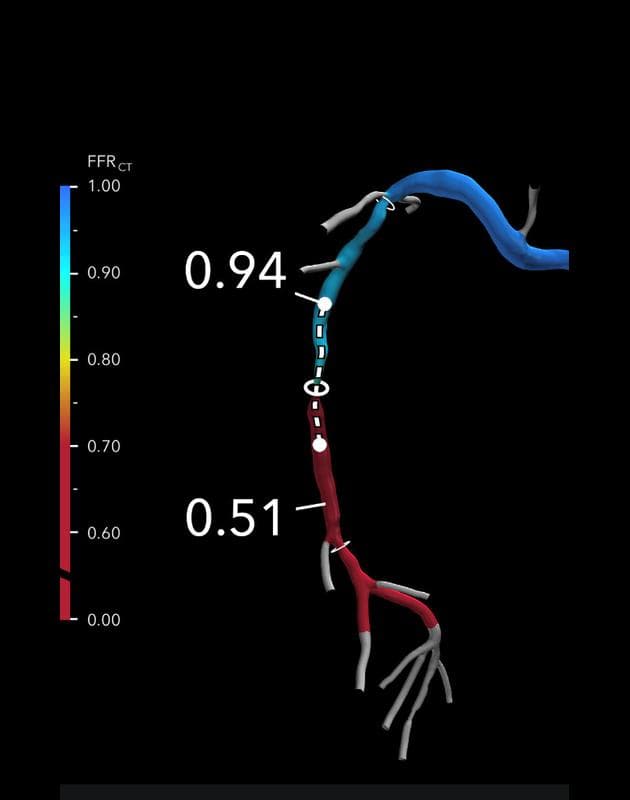
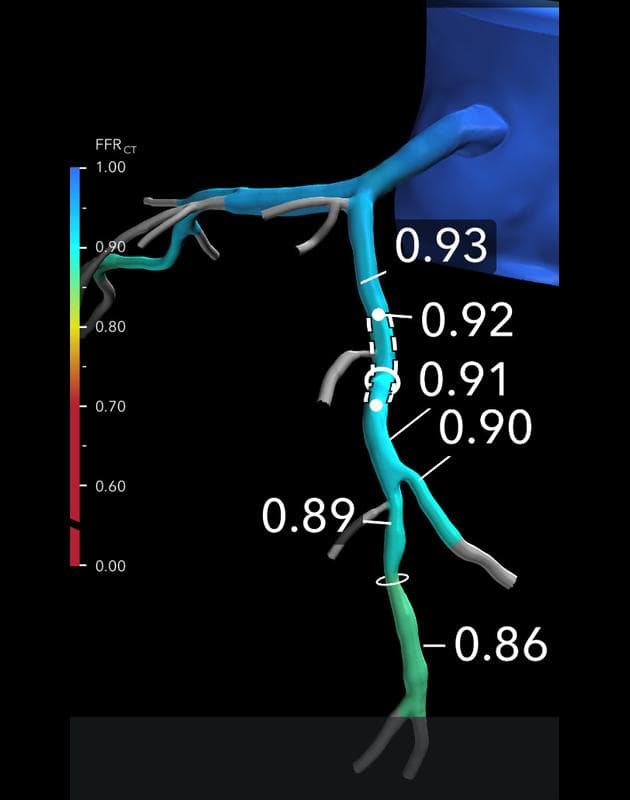
HeartFlow Planner - RCA
HeartFlow Planner was also used to gauge the potential impact of restoring the coronary lumen to its normal size.
Before
Before
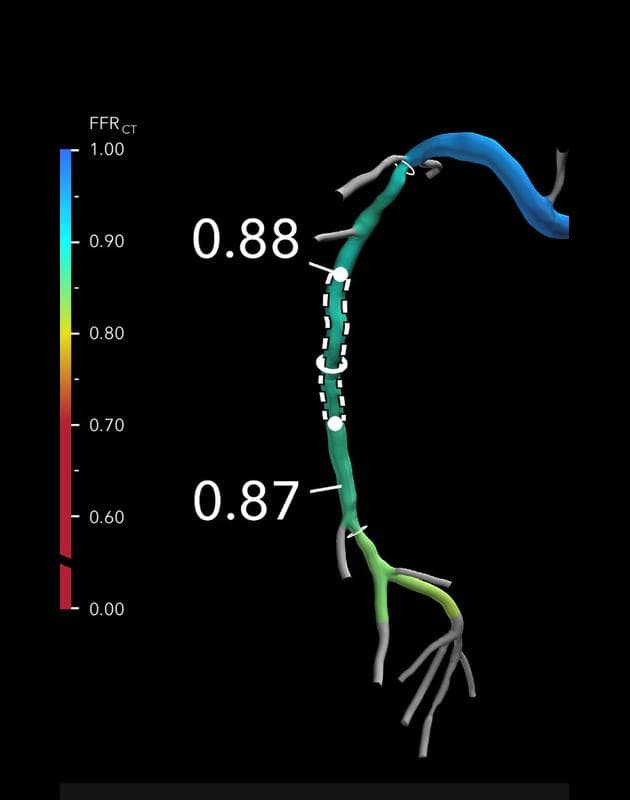
After
* HeartFlow Planner usage at Cone Health is part of a beta program. Not commercially available.
HeartFlow Planner - LCX
HeartFlow Planner was also used to gauge the potential impact of restoring the coronary lumen to its normal size.
Before
Before
After
* HeartFlow Planner usage at Cone Health is part of a beta program. Not commercially available.
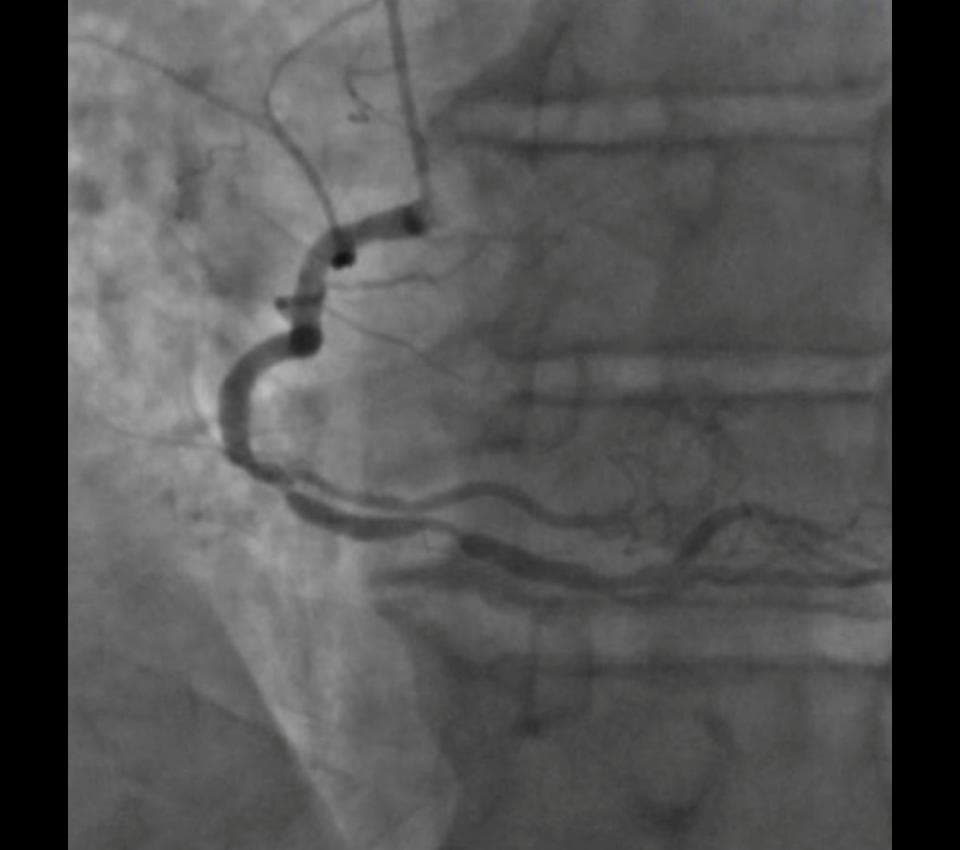
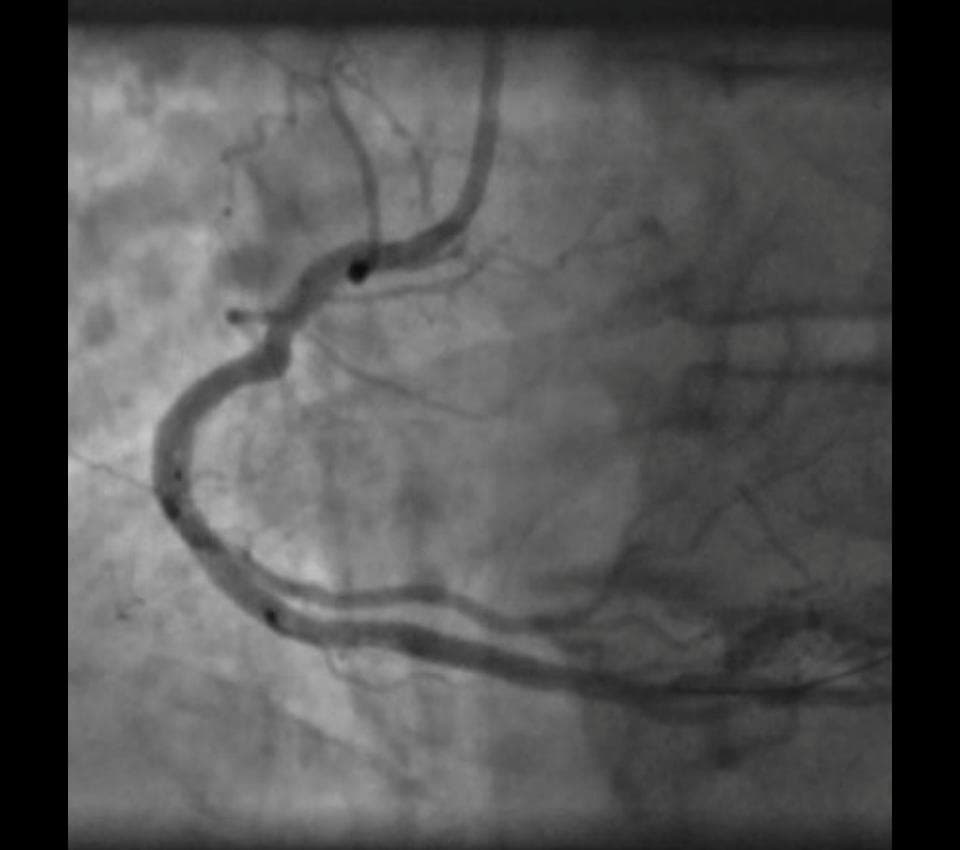
Angiography - RCA
Invasive coronary angiogram matched perfectly with the HeartFlow Analysis and HeartFlow Planner, which helped to identify the specific areas requiring intervention. Post PCI angio reflects unrestricted blood flow.
Before
After
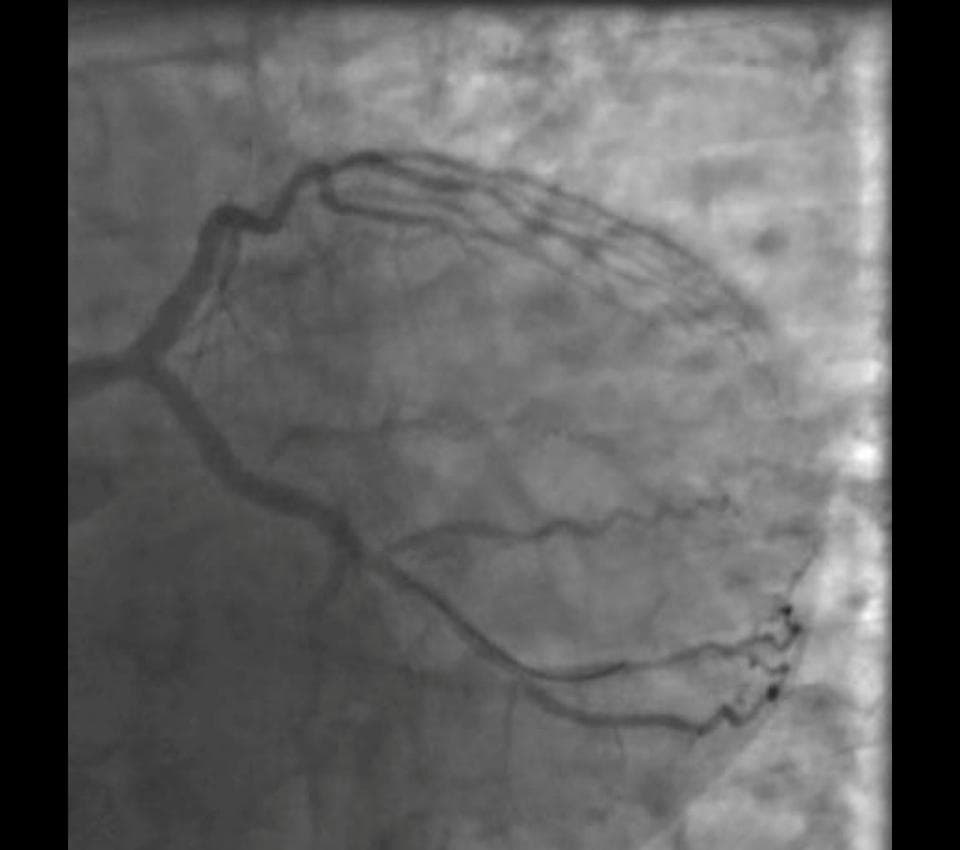
Angiography - LCX & LAD
The angio matched perfectly with the HeartFlow Analysis and HearFlow Planner, which helped to identify the specific areas requiring intervention. Post PCI angio reflects unrestricted blood flow.
Before
After
Results
Cardiac catheterization showed 80% stenosis in the mid RCA and 90% stenosis in the distal RCA; the patient received two drug eluting stents (DES) leaving 0% residual stenosis.
There was 75% stenosis in the proximal LCX artery, and the patient received a DES in this location. The patient received three stents in total.
The HeartFlow Analysis and HeartFlow Planner provided functional information to complement the anatomical findings in the CTA and provided guidance on how best to treat the patient prior to the procedure.
◀ Back
Next ▶
HeartFlow is available from anywhere
We have a comprehensive IT review process for vetting applications that go on mobile devices. Because of the ease of use and the security associated with it, we didn’t run into any major red flags. The approval actually went through smoother than others.
— Sheryl Booth, RT(R), MHA
Executive Director Heart & Vascular
I really like to have access on my phone — it expedites the process. I can quickly check on patients and text my colleagues if a patient needs to go to cath. It has nice features too — with a simple click you can see the FFRCT and different parts of the vessels.
— Katarina Nelson, MD
CT Program Lead, Imaging Cardiologist
My patients love to see their HeartFlow Analysis, and I always use my cell phone to show them.
— Henry Smith, MD
Interventional Cardiologist
I’ll read the CT interpretation and look at those photos and also log into the HeartFlow app and pull up the HeartFlow analysis to compare the two, learn the anatomy and correlate the diagnosis with the picture.
— Sara Wallace
Nurse Navigator
Key Benefits
to Cone Health
Improves diagnosis of coronary artery disease using CT + HeartFlow Analysis pathway
Supports continued CT program growth, plus improved CT reading and acquisition
Reduces high false positive diagnostic rates allowing for more appropriate use of the cath lab
Facilitates procedural and treatment planning for interventionalists
Simplifies workflows and improves efficiency
Enables meaningful patient interactions, education and engagement with HeartFlow mobile
“It really is a go to test, especially for the low-to- intermediate, but now also the higher risk patients, and it’s very accurate. So I love it! SPECT imaging is probably going to take a big hit in our institution.”
— Henry Smith, MD
of treatment plans changed after physicians evaluated patient care using the HeartFlow Analysis4
Adoption of the HeartFlow Analysis at Cone Health helped the team to further enhance their cardiac program — from growing their CCTA program to achieving greater cath lab efficiencies to strengthening team collaboration. Now with a growing CCTA program with expansion plans to include three scanning locations, eleven readers, and a growing network of referring providers, their passion for adopting advanced technology paired with a well-coordinated care team is a model of success. When administrator and physician goals are aligned, optimal patient care results.
Download mobile app
View PDF
Share with Email
Download our mobile app*, view a PDF of this page or share with a colleague by clicking above.
1. Arbab-Zadeh, Heart Int 2012. Yokota, et al. Neth Heart J 2018. Nakanishi, et al. J Nucl Cardiol 2016. 2. Patel, et al. N Engl J Med 2010. Patel, et al. AHJ 2014. Danad, et al. JAMA Cardiology 2017. 3. Hoffmann, et al. J Am Coll Cardiol. 2009. 4. Fairbairn, et al. Euro Heart J 2018. Patel, et al. JACC CV Imaging 2019.
*Mobile approval required by your institution to enable access.
Contact Us
*Required fields
Request the HeartFlow Analysis Near You
If you would like to request to have the HeartFlow Analysis available at a location near you, please submit your information below with details of the institution. We will share this information with the institution, but it will not guarantee HeartFlow will become available.
*Required fields
残念ながら、GDPR 規制により、この Web フォームを通じて求人への応募やキャリアに関する問い合わせを受け付けることはできません。弊社を通じてお申込みください 採用ページ. ご関心をお寄せいただきありがとうございます!
The HeartFlow FFRCT Analysis is a personalized cardiac test indicated for use in clinically stable symptomatic patients with coronary artery disease by qualified clinicians. The information provided by the HeartFlow Analysis is intended to be used by qualified clinicians in conjunction with the patient’s history, symptoms, and other diagnostic tests, as well as the clinician’s professional judgement.
If you have additional questions, close out of this message to complete our form or call our support team: 877.478.3569.
Please use our online submission form on the Clinical Research Page to apply for research grants.
Thank you for your interest!
Unfortunately, we cannot take job applications or career inquiries through this web form due to GDPR regulations. Please apply through our Careers Page. Thank you for your interest!
Campbell Rogers, M.D., F.A.C.C.
Executive Vice President and Chief Medical Officer
Campbell brings a wealth of experience to HeartFlow, where he serves as the Chief Medical Officer. Prior to joining HeartFlow, he was the Chief Scientific Officer and Global Head of Research and Development at Cordis Corporation, Johnson & Johnson, where he was responsible for leading investments and research in cardiovascular devices. Prior to Cordis, he was Associate Professor of Medicine at Harvard Medical School and the Harvard-M.I.T. Division of Health Sciences and Technology, and Director of the Cardiac Catheterization and Experimental Cardiovascular Interventional Laboratories at Brigham and Women’s Hospital. He served as Principal Investigator for numerous interventional cardiology device, diagnostic, and pharmacology trials, is the author of numerous journal articles, chapters, and books in the area of coronary artery and other cardiovascular diseases, and was the recipient of research grant awards from the NIH and AHA.
He received his A.B. from Harvard College and his M.D. from Harvard Medical School.